Humanising Digital Consent in Maternity Care

.png)

What did I do?
I collaborated with clinicians and parents to identify critical breakdowns in maternity care, translating these insights into scalable system journeys and service blueprints aligned with real clinical workflows. I designed trauma informed, enterprise ready digital experiences and validated them through iterative stakeholder feedback.
My role
Lead UI/UX and Service Designer
This included
• UX and content design
• Human AI interaction flows
• Visual and illustration system
• Prototyping using Figma, UX Pilot, Genially, Vibe Coding .
Duration - 3 Months
Problem Statement
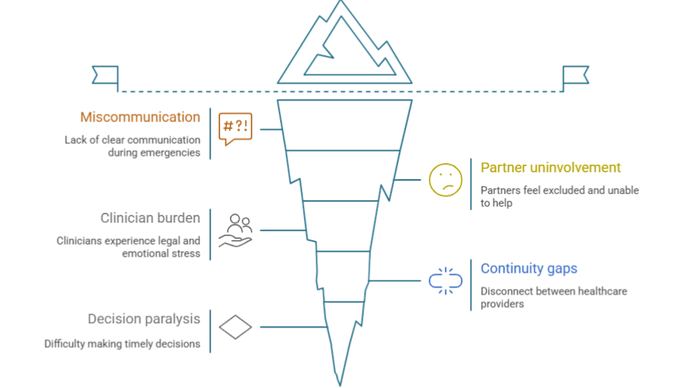
Consent during childbirth is often rushed, unclear, and emotionally overwhelming. Families frequently feel excluded from urgent medical decisions, unsure of what is happening or why.
70 %
Serious medical errors are associated with communication failures
33 %
36 %
36 %
Experience ongoing emotional distress linked to birth events
Women describe their birth as traumatic
Report consenting to interventions without fully understanding the risks
$20,000–$50,000
From a business perspective, each consent-related communication breakdown costs hospitals an estimated to resolve
Exposes organisations in potential legal liability per incident. (ACSQHC 2021; AHPRA 2022; Deloitte 2021; Victorian Ombudsman 2023)
$250,000–$500,000
300,000 births
Each year in Australia, Yet maternity care still runs on paper forms, disconnected systems.Source. Birth volume & national trends - AIHW “Australia’s mothers and babies” (annual report)
Solution
Re:Consent is a multi-layered consent system designed to reduce breakdowns in understanding, continuity, and trust across the maternity journey. Instead of treating consent as a one-time form, the system supports shared decision-making before, during, and after birth - when cognitive and emotional capacity change.
The solution intervenes at known failure points: early preparedness, time-critical decisions, information continuity across shifts, and post-birth emotional closure. Each layer is designed to reduce cognitive overload for families, save time for clinicians, and lower downstream risk for healthcare systems.






Antenatal Preparation Layer
What it does
Builds understanding before labour, reducing shock and fear during emergencies.
Root cause
Decisions are made under extreme pressure without clarity, agency, or emotional support. Consent is treated as a one-time form instead of an ongoing process.
Evidence
36% of women describe their birth as traumatic
Dynamic Intrapartum E-Consent Layer
What it does
Supports calm, structured decision-making during high-pressure moments with clear risks, benefits, and alternatives.
Root cause
-
Consent during emergencies is rushed, verbal, and poorly retained.
-
Parents often consent without fully understanding risks or options.
Evidence
36% of women report consenting to interventions without fully understanding the risks
Consent & Documentation hub
What it does
Creates a single source of truth for consents, preferences, and timelines across care teams and shift changes.
Root cause
Fragmented records and handovers cause repeated explanations, lost context, and documentation errors.
Evidence
70% of serious medical errors are linked to communication failures
(Safety in Health, BioMed Central)
Postnatal Reflection Layer
(AI-Enabled – AYLA)
What it does
Provides a trauma-informed, clinician-reviewed explanation of what happened and why, supporting emotional closure after birth.
Root cause
There is no patient-centred debrief after discharge.
Post-birth confusion becomes a silent failure once families leave the hospital.
Evidence
33% of women experience ongoing emotional distress linked to birth events
(Women’s Agenda)
View Project Impact
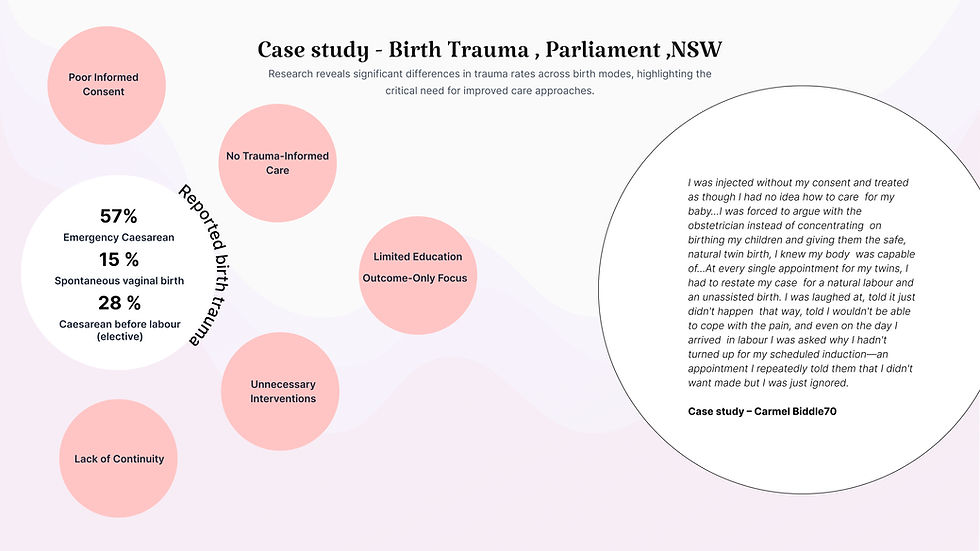
Birth Trauma - Visible Emotional distress after birth

How does this project bridge the gap?
By Restoring agency, trust, and emotional closure before , during and after birth..

Research shows most birth trauma stems from poor communication and lack of informed consent.

“We focus on consent because it is the leverage point that transforms communication, restores trust, and prevents trauma across maternity and beyond.”
Consent acts as the “moment of truth” where rights, trust, and care meet.
Health systems enforce safety protocols but neglect tools for shared decision-making and partner inclusion.
leverage point that improves communication, reduces trauma, and scales beyond maternity into surgery, emergency, and end-of-life care.
Discovery
I conducted a landscape analysis of global clinical standards, including WHO Quality of Care and NHS guidelines, which revealed a misalignment in maternity consent practices. Current tools like PDFs and generic birth plans fail to adapt to clinical changes, hinder shared decision-making, and lack follow-up after birth. Additionally, found fragmentation in technology across GP systems, hospital EMRs, and midwifery workflows.
So what is the Impact of Absent Shared Decision-Making,
Informed Decision-Making , Consent and lack of continuity in care in Maternity Care ?

Define
Through qualitative interviews with obstetricians, midwives, mothers, and partners, I surfaced deeper behavioural and emotional drivers. Themes included time scarcity, cognitive overload, lack of anticipatory guidance, and the absence of trauma informed communication. Importantly, I found that partners felt excluded and clinicians lacked tools that operationalise empathy within their time constraints. These insights informed a reframing of consent as an ongoing dialogue, not a one-time signature.
Opportunity to interview obstetricians.
the clinical director, and senior midwives at the Royal Women’s Hospital, meeting with them multiple times over three months. Alongside this, I interviewed mothers, partners, and CALD participants, analysed trauma reports, reviewed podcasts, and gathered insights from five close friends and family members. I also drew on my own lived experiences to deepen the research.
Interviews with mothers and Partners

-
Rushed or unclear communication: Mothers felt they had “no time to ask questions” — 73% felt rushed during 10–15 minute consults.
-
Emotional safety: Unclear or contradictory explanations caused anxiety — 9 out of 15 reported feeling unsafe.
-
Need for visual clarity: Visuals improved understanding — 12 out of 15 preferred diagrams and scenarios over text.
-
Partner involvement: Partner exclusion increased stress — 11 out of 15 wanted partners to receive the same explanations.
-
Difficulty processing birth events: Emergency decisions blurred memory — 80% couldn’t recall parts of labour.
-
Language + literacy barriers (CALD): Medical terms were overwhelming — all 5 CALD participants struggled with terminology.
-
No emotional closer during postnatal
Interviews with Clinicians & Midwives
-
Time pressure: Consults are too short for deep consent conversations - typically just 10–12 minutes.
-
Emergency limits: Consent is often rushed - decisions made in 5–20 minute windows
-
Need for visuals: Scenario-based consent reduces fear — clinicians prefer visual explanation tools.
-
Emotional labour load: Midwives bear the weight of reassurance — 60–70% of time spent on support and admin.
-
Reassurance over data: Tone matters more than facts — “Reassurance is 50 percent of care.”
-
Missing reflection: Postnatal debriefs are rare — only 0–1 structured sessions unless requested.
-
Trauma-informed need: Trust hinges on empathetic delivery — all midwives flagged tone as critical.

Research Highlights (From Field Interviews)
Even advanced platforms - EIDO, Concentric, TeamBirth, Babyscripts remain siloed. They address single slices, not the full journey.
This lack of continuity is the leverage point I focused on: closing the loop and turning fragmented touchpoints into a connected, reassuring care experience that supports both emotional well-being and informed decision-making throughout the entire journey.























This creates a fragmented experience. Families get information in disconnected bursts, with no emotional or informational clarity across the journey.
Antenatal → PDFs for education
Intrapartum → Consent forms during labour
Postnatal → EMR notes
Current tools only cover isolated moments:
The Gap: Fragmented and Systemic Break in Maternity Care
How might we reimagine maternity consent as a continuous, trauma-informed journey , preparing mothers and partners in advance, supporting them in the moment, and ensuring clarity and trust after birth?
Define + Opportunity Space
“When I synthesised the thematic insights from mothers, partners, obstetricians, and midwives, I realised that the core problem was not lack of information but lack of emotionally safe, continuous, and shared communication. Consent was happening too late, too fast, and too narrowly reduced to signatures rather than understanding. Each insight exposed a structural gap: rushed appointments, fragmented explanations, partners excluded, and no postnatal reflection. These became the foundation of Re:Consent. From this analysis, the opportunity space became clear. I saw the need to shift consent upstream into antenatal care where decisions can be practised before stress sets in. I recognised that transparency must be built into the entire system, not just a single touchpoint. And I understood that any solution must work within 10-minute appointments while still supporting deep emotional needs. By reframing consent as a continuous journey rather than a one-off moment, I could design a service that strengthens shared decision making, rebuilds trust, and supports families across antenatal, intrapartum, and postnatal care. This opportunity space positioned Re:Consent as a bridge between empathy and efficiency, aligning with WHO respectful maternity care standards and the BRAIN framework for informed birth decisions. Re:Consent ultimately emerges from this insight: when communication becomes clear, structured, and trauma-informed, consent transforms from a rushed obligation into a shared safeguard that empowers mothers, partners, and clinicians alike.”








Develop
Through I prototyped an integrated service ecosystem that reframes consent as a continuous, connected, and emotionally safe experience. The solution comprises four core components: early-stage learning modules that scaffold understanding,
a dynamic e-consent tool that supports real-time decision-making, a unified document hub that enhances continuity across touchpoints, and an AI-generated reflection kit that guides structured postnatal debriefing.
Expletory design development
Before beginning the Re:Consent project, my approach was intentionally broad and exploratory. Initially, I envisioned creating a physical intervention something tactile that could exist within hospitals to support communication and consent. This early phase focused on “brain-to-hand” design through sketches and paper-based prototyping to visualise the maternal care journey. However, as the exploration progressed, several practical limitations emerged. Physical artefacts within hospital environments presented significant hygiene and management challenges, and maintaining cleanliness across shared objects became unrealistic in postnatal and labour settings. Through conversations with peers and clinical references, I also identified a recurring pain point: mothers and families are already overwhelmed by numerous physical materials such as brochures, consent papers, and printed guides. These are often fragmented, easily lost, and rarely revisited. As the healthcare system moves toward digitisation of records and education, it became evident that a digital solution would provide more flexibility, continuity, and accessibility. I therefore transitioned the concept into a digital design space, allowing for iterative refinement and real-time adaptability. Early journey maps and consent flows were still hand-drawn on paper to establish logic and narrative clarity. Once the structure was validated, I developed a digital prototype, which proved easier to iterate, manage, and integrate with existing hospital systems. This shift from physical to digital not only improved practicality but also aligned with contemporary trends in connected, trauma-informed healthcare design.













As the project grew in complexity, I structured Re:Consent as a single service system rather than isolated features. I mapped key breakdown points across pregnancy where anxiety is high, time is limited, and consent often becomes unclear. This led to design a three-phase framework aligned with how people actually experience care: before, during, and after birth.
The framework adapts interactions to users’ cognitive and emotional capacity at each stage. Visual walkthroughs support preparation before birth, critical prompts reduce decision fog during birth, and the Reflection Kit provides closure after birth.
This structure guided all UI decisions and system flows, ensuring clarity, empathy, and shared decision-making throughout the journey.
AI-Assisted Vibe coding and UX Workflow
To accelerate a complex project with many clinical pathways, I used AI as a UX pilot while keeping full control of the design direction. I first defined the system framework and information architecture for Re:Consent, then used a master prompt (“vibe code”) to generate early content for scenarios and screens. AI often produced excess or misaligned information, so I curated and refined it carefully. Around 60 percent of the generated content was usable after restructuring it into my trauma-informed IA. This workflow helped me manage time under a tight deadline while still designing clear, human-centred interfaces across high-pressure procedures such as NIPT, amniocentesis, emergency C-section and stillbirth care.
Designing a Trauma-Informed Prototype to Reduce Decision Fog


From Framework to Journey Touchpoints and Blueprint
I started by structuring the system through a service framework and then used journey mapping to identify emotional and operational breakdowns. I translated these insights into a service blueprint so the UI reflected real clinical workflows and constraints rather than speculation. This progression from service framework → journey mapping → service blueprint → UI ensured every design decision was operationally grounded, scalable, and clinically viable.







Why the Concept of Agentic AI Emerged
While mapping the maternity care journey, I identified a systemic gap: consent is documented ( Manually or diary writing ), but understanding and emotional closure are not supported,( No one is closing the loop ) especially after emergencies and shift changes.
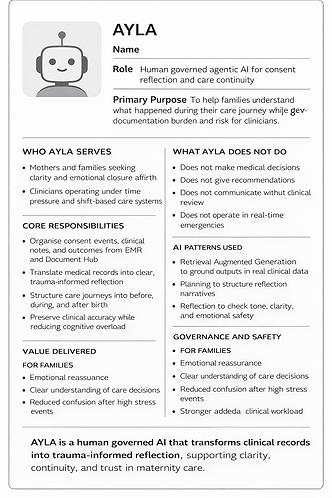
I designed AYLA, a human-governed agentic AI that translates existing clinical records into a trauma-informed reflection, reviewed by clinicians before release. AYLA reduces cognitive overload for families and documentation burden for clinicians, improving continuity, trust, and risk outcomes at scale.
Solution Overview - Make consent calm, continuous, and collaborative.
Antenatal Preparation Layer
1
Prevent breakdowns before they happen
This layer prepares parents before decisions occur, when learning capacity is highest and anxiety is lower. By shifting education upstream, it reduces pressure on families and clinicians during high-risk moments.
Design Principle - Design for the option to ask, not the pressure to speak.
What it is
What It Solves
What It Includes
Impact At a Glance
Business Impact
Prepare parents before decisions occur when learning capacity is highest and anxiety is lower
Problems addressed
-
Parents unprepared for critical decisions
-
Consent conversations rushed under pressure
-
Partners unclear on how to support
-
Anxiety escalates during emergencies
This reframes the feature as a system fix, not a learning tool.
-
Flip-and-Learn visual modules
-
What-if scenario walkthroughs
-
Partner prompt scripts
-
scan, amniocentesis)
Procedure explanations
(NIPT, 8–12 week
-
Partner enablement effect
Measured impact
-
5–10 minutes saved per critical consent discussion
-
1–2 fewer clarification loop per birth
-
15–30% fewer decision- question during during and after birth
-
Reduced anxiety-driven escalation in emergencies
Why this matters at system level
-
Reduced clinician time spent re-explaining procedures
-
Faster consent alignment during labour
-
Lower documentation and consent-related risk
-
Improved care efficiency without increasing appointment time
-
Higher perceived quality of care and patient trust

Learning Modules - Scenario-Based Education
Interactive flip cards and “What-if” walkthroughs prepare parents for real decisions before labour begins. They replace overwhelming PDFs with calm, visual learning - empowering both parents to engage early and equally.
Using AI for Content Development
To build consistent, trauma-informed content, I used GPT and RMIT’s VAL platform as part of a structured writing workflow. I designed prompts that aligned with clinical guidelines and decision-making frameworks, then refined AI-generated text through human judgment and research. Across all modules, I created twelve decision trees and used AI to help organise tone, flow, and clarity — but I kept all final decisions grounded in ethics, accuracy, and lived experience insights.
User Interface Reflection
Designed the interface to lower cognitive load and reduce anxiety. The visual hierarchy is soft and simple, and the line drawing illustrations help keep the experience grounded without feeling clinical. I used long-scroll pages instead of multi-step clicking because it lets users follow the story at their own pace. The decision tree, Q&A blocks, and conversation prompts give both mother and partner a structured way to understand options and prepare for discussions with clinicians.
I designed the learning modules to cover the full maternity journey, but I intentionally focused on the moments where communication breaks down most. After mapping all antenatal, intrapartum, and postnatal procedures, I narrowed the scope to the high-stakes points clinicians and mothers identified as the most confusing: NIPT, amniocentesis, instrumental delivery, emergency caesarean, stillbirth, feeding choices, and contraception after birth. To keep information consistent, I applied the NHS BRAIN framework — Benefits, Risks, Alternatives, Intuition, and Next or Nothing and developed an information architecture framework for this project according to pain points and needs... This gave every module a clear rhythm and helped me translate clinical complexity into calm, trauma-informed, and emotionally safe content for both mothers and partners.
Why This Approach Works
By narrowing the scope to the most emotionally fragile moments, and pairing it with trauma-informed language, clear IA, and structured decision-making support, I transformed overwhelming clinical procedures into calm, human, and accessible guidance. This approach keeps the system usable for families, feasible for clinicians, and scalable across any future medical procedure.
Information Architecture (IA)
I structured each procedure page to feel predictable and supportive: • Header: simple navigation for Home, Procedures, Mother View, Partner View • Overview: a short, empathetic explanation of the procedure • Summary Cards: what it is, why it happens, consent types • Decision Tree: shows how choices unfold in real time • Care Information: before, during, and after the procedure • BRAIN Framework: clear benefits, risks, and alternatives • Emotional Experience: mother and partner perspectives • Recovery: practical timelines and safety guidance • Conversation Prompts: questions to ask clinicians • Illustrations: minimal, calm visuals to reduce stress This structure allowed me to hold emotional complexity while keeping the experience extremely clear.

Dynamic Intrapartum E-Consent Layer
2
Support decisions under pressure
A digital walkthrough that simplifies urgent consent moments, showing why, risks, alternatives, and time window instantly.
Ensures ensures mothers voice remains central even under stress
Design Principle - Design for clarity when time and cognition are limited.
Consent must adapt to pressure, not add to it.
What it is
A time-aware digital consent flow used during labour when time is limited and cognitive load is high. It simplifies complex decisions into clear, actionable steps without removing patient control.
What It Solves
Problems addressed
-
Rushed verbal consent during emergencies
-
Long explanations that are hard to process under pain or stress
-
Partners unsure how to support or act as proxies
-
Anxiety escalation during critical moments
What It Includes
-
Emergency e-consent screens
-
Time-window prompts for urgent decisions
-
Clear procedure explanations
-
Midwife-facing view linked to EMR
-
Clear visibility of time-sensitive options
Impact At a Glance
Measured impact
-
3–7 minutes faster consent alignment during emergencies
-
20–40% reduction in repeated verbal explanations
-
100% auditable e-consent events
-
Lower cognitive load for clinicians under pressure
Business Impact
-
Faster emergency decision throughput
-
Reduced consent-related risk and disputes
-
Improved documentation quality under stress

Document Hub
3
Preserve continuity across shifts
A unified digital space linking GP, hospital, and family. keeping every signed form and summary in one accessible hub.
It reduces duplication, confusion, and lost communication between care teams and parents.
Design Principle - Continuity builds trust when care is shared.
What it is
A central, shared space for all consent-related records, preferences, and updates across the maternity journey.
What It Solves
Problems addressed
-
Information loss during shift changes
-
Fragmented consent records across systems
-
Parents unable to track decisions or updates
-
Partners excluded from shared understanding
What It Includes
-
Signed consents and refusals
-
Preferences and notes
-
Timeline of updates
-
Optional partner access
Impact At a Glance
Measured impact
-
1–3 fewer repeated explanations per patient across care teams
-
5–8 minutes saved per handover during shift changes
-
20–30 percent reduction in time spent re-locating consent and preference information
-
15–25 percent reduction in documentation errors linked to fragmented records
Business Impact
-
Reduced clinician rework
-
Lower documentation and compliance risk
-
Improved operational efficiency

Postnatal Reflection Layer (AI-Enabled – AYLA)
4
Closure and understanding after care
Two weeks after birth, an AI agent -Ayla compiles the care journey in gentle, trauma-informed language for parents to reflect on.
It closes the emotional loop of care -transforming medical data into understanding, healing, and trust.
Design Principle - Understanding after care is as important as consent during care.
What it is
An AI-supported Reflection Kit that explains what happened and why, reviewed
What It Solves
Problems addressed
-
Post-birth confusion after complex or emergency care
-
No patient-centred debrief (discharge summaries are clinical, not explanatory)
-
Lack of emotional closure after high-stress birth events
What It Includes
-
Plain-language explanations
-
Birth timeline Decision explanations
-
Trauma-informed language
-
Human review workflow
-
Guidance for parents
Impact At a Glance
Measured impact
-
30–50 percent reduction in silent post-discharge confusion
-
1 fewer follow-up call or appointment triggered by uncertainty per family on average
-
Improved patient understanding and recall of birth events
Business Impact
-
Reduced documentation and medico-legal risk through clearer, patient-centred summaries
-
50 percent reduction in post-discharge clarification requests by addressing silent failure in understanding
• Lower clinician time loss
AI Agent Impact – AYLA
Converts fragmented clinical data into governed summaries that reduce follow-up workload, lower documentation risk, and scale continuity without increasing clinician time.
Clinical View - Back stage

New Parents View - Front stage

Project Impact: Delivering Value to Users and Businesses
To validate the research and design innovation of Re:Consent, I conducted prototype testing with the Royal Women’s Hospital team, including Dr. Julia Unterscheider (Obstetrician) and Nova Barrios (Midwife).
Clinical -Validation

Positive feedback around tangible benefits: reduces stress, and supports safer, personalised care during pregnancy
80%
-
“The Reflection Kit and partner prompts are brilliant”
-
“We need empathetic tools like this in maternal health”
-
“It has emotional depth and real world practicality”
-
“Simple, dynamic, and genuinely meaningful for patients”
-
“Well developed and ready to evolve further”

Reflection kit
Prompts cards for each procedure

Potential to impact 70 % Potential to impact 900+ staff annually in Royal Women’s Hospital alone.
Digital healthcare adoption can save $5.4B/year in efficiency and duplication costs

User Testing
Re:Consent was evaluated with participants across multiple age groups and life stages, including future parents, partners, and older caregivers. The system demonstrated strong alignment with enterprise healthcare goals of clarity, inclusion, and continuity.
30s
Mid-aged participants described it as clear, empathetic.
-
“The tone makes it clear how I can support without overstepping.”
-
“It shows what to ask, even when you don’t know where to start.”
60s
20s
Reflected that it reintroduced a sense of community and shared care missing in today’s individualised society in maternal health .
-
“Birth used to be a shared, community experience.”
Younger participants (20–27) found it emotionally engaging and empowering
-
“I rated this 10 out of 10. I wish I had known these questions back then.”
-
“At first I thought this was only for women. Now I see how I can participate.”
From Interface Design to System Responsibility
Critical Reflection
Re:Consent reframed consent from a one-time interaction to a continuous, shared responsibility. The project shifted my focus from interface design to system safety, trust, and governance. I learned that effective service design must balance emotional complexity, clinical reality, and responsible AI to support informed, shared decision-making.
Transferable Design Strengths
-
Streamlined complex workflows across fragmented stakeholders
-
Designed governed, human-in-the-loop AI within regulated environments
-
Synthesised needs of patients, partners, clinicians, and systems
-
Designed frameworks that scale beyond a single domain or interface.
Design Principles That Emerged
-
Design for safer conversations, not smoother screens
-
Use plain, empathetic language to reduce cognitive load
-
Support shared decision-making, not medical recommendations
-
Build trust through transparency, choice, and continuity
-
Good AI is not smarter, it is safer and more responsible
-
No opt-out equals poor user control
-
No memory controls equals loss of trust
-
Close collaboration with midwives and obstetricians was essential. It taught me how healthcare systems actually operate, how trust is built or broken, and why responsibility matters more than novelty when designing for real-world impact.